All published articles of this journal are available on ScienceDirect.

Sex Differences in the Effects of a Biological Drug for Rheumatoid Arthritis on Depressive State
Authors Info & Affiliations
Abstract
Objective :
Sex-specific medicine has attracted attention in recent years, but no report on rheumatoid arthritis (RA) has examined sex differences in the effectiveness of biologics on activities of daily living (ADL), quality of life (QOL), or depressive state.
Methods :
The study subjects were 161 RA patients (female: 138; male: 23) attending regular doctor visits at our hospital. We compared the changes in disease activity, which was evaluated using the simplified disease activity index (SDAI), ADL (using the modified health assessment questionnaire; mHAQ), QOL (using short form-36; SF-36), and the Hamilton Depression Rating Scale (HAM-D) for RA patients between each sex over a six-month observation period while administering biologic treatment.
Results :
The female patients reported significant improvements in the following metrics: SDAI: from 22.1 ± 11.9 to 8.9 ± 7.8 (p < 0.001); mHAQ: from 0.46 ± 0.50 to 0.32 ± 0.45 (p < 0.001); and HAM-D: from 6.2 ± 4.8 to 3.8 ± 4.1 (p < 0.001). Moreover, all eight items of the SF-36 were significantly improved (p < 0.01). In contrast, the male patients improved on the SDAI (from 27.9 ± 11.7 to 12.7 ± 8.6 (p < 0.001)), but we did not observe significant improvements in the mHAQ or HAM-D scores or in any items on the SF-36.
Conclusion :
Both male and female patients with RA improved when using a biological drug. Sex differences in the improvement of depressive state were observed.
INTRODUCTION
Rheumatoid arthritis (RA) is a disease characterized by chronic pain. RA affects activities of daily living (ADL) by causing joint destruction/deformation, reduces quality of life (QOL), and is associated with psychological disorders, particularly depression [1-3]. Among the various complications of RA, depression is the most common, affecting approximately 20% of RA patients [3]. Factors related to depression include social factors, sex, age, race, functional disorders, and disease activity level [4].
Treatment for RA has changed greatly over the last 10 years. The therapeutic goal has been clarified as “treat to target” (T2T). Among RA treatments, methotrexate (MTX) has firmly gained ground as an anchor drug. Furthermore, it is recommended to actively use a biological drug when MTX displays insufficient efficacy for T2T [5].
Biological drugs have rapid therapeutic effects and show high effectiveness, even in RA cases in which MTX has been ineffective. In addition, the goal of RA treatment in terms of T2T has shifted from clinical remission and controlling ordinary disease activity to imaging remission, as measured by X-rays, or functional remission, as measured by QOL. There have been increasing numbers of reports of complete remission, as defined by multiple measures (clinical, imaging, and functional remission). However, female sex, current smoking, positivity for autoantibodies against rheumatoid factor or CCP, a long disease duration at the time of treatment initiation, and depression are adverse prognostic factors [6].
We have previously reported that depression in RA patients can be improved via infliximab and etanercept treatment [7]. In addition, we have reported on the extent of the effects of biological drugs, except for infliximab and etanercept, on physical function and on the improvement of depression. Sex-specific medicine has attracted attention recently. Female is an adverse prognostic factor for RA patients. A number of reports have compared the differences in the drug effects on RA [8-10], ADLs and QOL between each sex; however, we could not find reports limited to biological drugs or reports comparing and examining depressive states. Therefore, we compared the sex differences in depressive state among RA patients treated with a biological drug.
MATERIALS AND METHODS
We used a cohort study design. We conducted the study at a single facility in the Division of Rheumatology, Department of Medicine, Showa University School of Medicine. The study period was set from November 1, 2005, to December 31, 2012, and patients who began treatment with a biological drug were registered during this period. Of the 184 RA patients using one of 6 biological drugs, we selected 161 RA patients (female: male = 138:23) for analysis. The observation period was set at six months. The biological drugs used in the study were infliximab (54 patients), etanercept (21 patients), adalimumab (30 patients), tocilizumab (30 patients), abatacept (20 patients), and golimumab (six patients). There were no patients using certolizumab pegol. There was no significant difference in ADL, QOL, or depressive state between the patients according to the type of biologic treatment. Therefore, we examined all such treatments together. We left the selection of biological drugs to the discretion of the doctor in charge. We reviewed or examined the following items before the initiation of treatment and at six months after treatment: age, sex, disease duration, steroid dosage, and MTX dosage. We used the Simplified Disease Activity Index (SDAI) as a disease activity measure for RA [11]. We also used a modified health assessment questionnaire (mHAQ) [12] as an ADL evaluation measure for RA patients and used short form (SF)-36 [13] as a non-specific health-related QOL evaluation. The Hamilton Depression Rating Scale (HAM-D) was used as an evaluation of depressive state [14]. We did not set limitations on the dosage or use/non-use of anti-rheumatoid drugs, adrenocortical steroids, or non-steroidal anti-inflammatory drugs before the initiation of treatment. We also did not set limitations on progressive reduction/ withdrawal of adrenocortical steroids or non-steroidal anti-inflammatory drugs.
The primary outcome measures were clinical efficacy, ADL, non-specific health-related QOL, and depressive state. The score for each item before/after the initiation of treatment was analyzed by sex. Paired t-tests, Student's t-tests, χ2 tests, the Mann-Whitney U test, logistic regression analysis, the Wilcoxon signed-rank test and repeated-measures analyses of variance were used for statistical analysis. In addition, the execution, analysis, and exami-nation of the HAM-D was conducted under the instruction of SK. Exclusion criteria included the following: use of antidepressant drugs at the time of treatment initiation or during the testing period; withdrawal of the biological drug due to the lack of an effect or adverse effects; additional internal use of anti-rheumatoid drugs and steroid/non-steroid anti-inflammatory drugs; development of complications other than depression, such as infectious disease; treatment discontinuation due to a hospital transfer or any other reason; request by the patient to withdraw from the study; and determination as inappropriate by the doctor in charge. Because most of the complications were infections that required hospitalization and because no cases restarted biologicals during the study period, we applied these exclusion criteria. The statistical software used was JMP10 (2012 SAS Institute, Inc.).
We acquired written informed consent from all patients enrolled in the study. Furthermore, the study received approval from the Bio-Ethics Committee of the Department of Medicine, Showa University School of Medicine.
RESULTS
The total size of the study cohort was 184 patients. We considered 161 patients to be valid analytical subjects but excluded 23 patients for the following reasons: seven patients dropped out of the study due to the development of complications, such as infectious disease requiring hospitalization; five patients dropped out due to primary failure of the drug; four patients transferred from the hospital; three patients asked to withdraw from this study; two patients stopped visiting the hospital; one patient canceled the test due to being unable to pay for the drugs; and one patient lacked data (Fig. 1). In addition, we did not find the following cases in this study: cases using antidepressant drugs at the time of initiation of treatment or during the study period; cases experiencing secondary drug failure; cases with direct adverse effects of the drug; or cases with additional internal use of anti-rheumatoid drugs or steroid/non-steroid anti-inflammatory drugs.
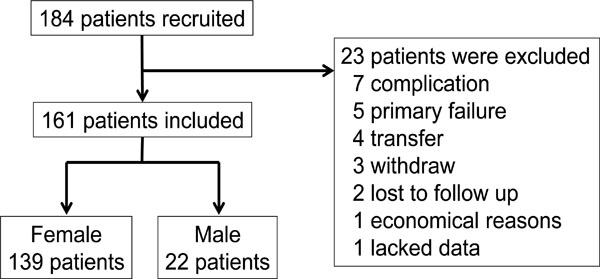
Flow chart of the study.
The patient cohort consisted of 138 female and 23 male subjects. The age at the time of biological drug initiation tended to be older for male subjects, but this difference was not significant (p=0.162). The dosage of steroid/MTX was higher for male subjects than for female subjects. Women had a longer disease duration than men (p=0.049) (Table 1).
Baseline characteristics of the patients.
| Univariate Analysis | Multivariate Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Female | Male | p | p | Odds Ratio | 95% CI | ||
| n | 138 | 23 | |||||
| Age (years) | 59.3 ± 14.7 | 63.9 ± 11.8 | 0.162* | ||||
| Disease duration (years) | 7.7 ± 8.2 | 4.2 ± 2.8 | 0.049* | ||||
| Steroid dosage (mg/d) | 2.9 ± 3.1 | 5.0 ± 3.4 | 0.005* | 0.124 | 1.189 | 0.954-1.482 | |
| MTX dosage (mg/w) | 8.2 ± 4.0 | 5.8 ± 4.4 | 0.011* | 0.118 | 0.866 | 0.724-1.037 | |
| Infliximab | 50 | 4 | 0.42** | ||||
| Etanercept | 14 | 7 | |||||
| Adalimumab | 24 | 6 | |||||
| Golimumab | 6 | 0 | |||||
| Tocilizumab | 28 | 2 | |||||
| Abatacept | 17 | 3 | |||||
| SDAI | 22.1 ± 11.9 | 27.9 ± 11.7 | 0.036* | ||||
| mHAQ | 0.46 ± 0.50 | 0.59 ± 0.48 | 0.257* | ||||
| HAM-D | 6.2 ± 4.8 | 5.8 ± 4.3 | 0.724* | ||||
| HAM-D>7 | 31 (22.5%) | 1 (4.3%) | 0.045*** | 0.011 | 0.041 | 0.004-0.486 | |
| SF-36 | Physical functioning | 29.3 ± 17.6 | 25.8 ± 17.7 | 0.335* | |||
| Role function (physical) | 31.9 ± 16.1 | 28.7 ± 15.6 | 0.385* | ||||
| Pain | 35.6 ± 9.1 | 33.2 ± 8.6 | 0.252* | ||||
| General health perception | 39.0 ± 9.1 | 34.8 ± 8.1 | 0.040* | ||||
| Fatigue | 43.2 ± 11.5 | 41.2 ± 10.9 | 0.426* | ||||
| Social functioning | 40.3 ± 14.7 | 36.4 ± 15.7 | 0.254* | ||||
| Role function (emotional) | 38.9 ± 16.3 | 33.8 ± 16.4 | 0.171* | ||||
| Mental health | 46.6 ± 11.2 | 39.2 ± 11.1 | 0.005* | 0.006 | 0.895 | 0.826-0.968 | |
Mean ± standard deviation.
SDAI: Simplified Disease Activity Index.
mHAQ: modified health assessment questionnaire.
HAM-D: Hamilton Depression Rating Scale.
SF-36: short form-36.
* analysis using Student's t-test.
** analysis using the χ2 test.
*** analysis using the Mann-Whitney U test.
Clinical characteristics according to sex before and after treatment.
| Female | Male | |||||||
|---|---|---|---|---|---|---|---|---|
| 0 Weeks | 6 Months | p | 0 Weeks | 6 Months | p | |||
| SDAI | 22.1 ± 11.9 | 8.9 ± 7.8 | 0.000* | 27.9 ± 11.7 | 12.7 ± 8.6 | 0.000* | ||
| mHAQ | 0.46 ± 0.50 | 0.32 ± 0.45 | 0.000* | 0.59 ± 0.48 | 0.43 ± 0.62 | 0.166* | ||
| HAM-D | 6.2 ± 4.8 | 3.8 ± 4.1 | 0.000* | 5.8 ± 4.3 | 4.8 ± 3.9 | 0.148* | ||
| HAM-D>7 | 31 (22.5%) | 15 (10.9%) | 0.000** | 1 (4.3%) | 5 (21.7%) | 0.317** | ||
| SF-36 | Physical functioning | 29.3 ± 17.6 | 36.1 ± 17.2 | 0.000* | 25.8 ± 17.7 | 29.4 ± 16.2 | 0.122* | |
| Role function (physical) | 31.9 ± 16.1 | 38.0 ± 15.1 | 0.000* | 28.7 ± 15.6 | 32.8 ± 14.9 | 0.182* | ||
| Pain | 35.6 ± 9.1 | 41.4 ± 9.4 | 0.000* | 33.2 ± 8.6 | 37.6 ± 10.6 | 0.065* | ||
| General health perception | 39.0 ± 9.1 | 42.9 ± 9.8 | 0.000* | 34.8 ± 8.1 | 36.0 ± 7.4 | 0.293* | ||
| Fatigue | 43.2 ± 11.5 | 47.1 ± 11.0 | 0.000* | 41.2 ± 10.9 | 43.4 ± 10.6 | 0.207* | ||
| Social functioning | 40.3 ± 14.7 | 45.0 ± 12.4 | 0.000* | 36.4 ± 15.7 | 38.6 ± 13.4 | 0.272* | ||
| Role function (emotional) | 38.9 ± 16.3 | 42.6 ± 15.1 | 0.000* | 33.8 ± 16.4 | 37.3 ± 14.4 | 0.236* | ||
| Mental health | 46.6 ± 11.2 | 49.6 ± 10.5 | 0.000* | 39.2 ± 11.1 | 41.4 ± 10.8 | 0.260* | ||
Mean ± standard deviation.
SDAI: Simplified Disease Activity Index.
mHAQ: modified health assessment questionnaire.
HAM-D: Hamilton Depression Rating Scale.
SF-36: short form-36.
* analysis using the paired t-test.
** analysis using the Wilcoxon signed-rank test.
Difference between female and male subjects and between before and after treatment.
| Females vs Males | Before vs After Treatment | Interaction | ||
|---|---|---|---|---|
| SDAI | 0.011 | 0.000 | 0.468 | |
| mHAQ | 0.277 | 0.000 | 0.937 | |
| HAM-D | 0.868 | 0.000 | 0.624 | |
| HAM-D>7 | 0.301 | 0.005 | 0.000 | |
| SF-36 | Physical functioning | 0.145 | 0.000 | 0.403 |
| Role function (physical) | 0.171 | 0.000 | 0.599 | |
| Pain | 0.085 | 0.000 | 0.567 | |
| General health perception | 0.003 | 0.000 | 0.211 | |
| Fatigue | 0.197 | 0.000 | 0.511 | |
| Social functioning | 0.056 | 0.000 | 0.429 | |
| Role function (emotional) | 0.139 | 0.004 | 0.786 | |
| Mental health | 0.001 | 0.000 | 0.737 | |
SDAI: Simplified Disease Activity Index.
mHAQ: modified health assessment questionnaire.
HAM-D: Hamilton Depression Rating Scale.
SF-36: short form-36.
Analysis using repeated-measures ANOVA.
There was no significant difference in the biological drugs used between the sexes (p=0.42). The disease activity of RA before treatment initiation was higher for male subjects. Nevertheless, there were no sex differences in ADL or depressive state. Regarding the items on the SF-36, a non-specific health-related QOL evaluation, two items, “general health perception” and “mental health”, were higher for female subjects than for male subjects at the time of the treatment initiation (p<0.05). Although we detected a significant difference only in HAM-D> 7 and the “mental health” item of the SF-36, no significant difference in disease duration, the SDAI score, steroid dosage or MTX dosage was detected based on multivariate analysis.
The SDAI score significantly improved for both female (from 22.1 ± 11.9 to 8.9 ± 7.8 [p=0.000]) and male subjects (from 27.9 ± 11.7 to 12.7 ± 8.6 [p=0.000]). The mHAQ significantly improved for female subjects (from 0.46 ± 0.50 to 0.32 ± 0.45 [p=0.000]) but not male subjects, despite a decreasing trend (from 0.59 ± 0.48 to 0.43 ± 0.62 [p=0.166]). The HAM-D score was significantly improved for female subjects (from 6.2 ± 4.8 to 3.8 ± 4.1 [p=0.000]) but not for male subjects (from 5.8 ± 4.3 to 4.8 ± 3.9 [p=0.148]). Female subjects showed a significant improvement in all 8 categories on the SF-36 (p=0.000). In contrast, male subjects did not show a significant improvement in any of the items (Table 2).
Next, we compared the outcome measures between before and after treatment and between the sexes via repeated-measures analysis of variance (Table 3). We found a significant improvement in all of the items on the SDAI, the mHAQ, and the HAM-D (p=0.000). However, in the comparison between sexes, there was a significant improvement in the SDAI, but not the mHAQ or the HAM-D. Although there was a significant improvement in all of the items of the SF-36 from before treatment to after treatment (p=0.011), only two items, “general health perception” (p=0.003) and “mental health” (p=0.001), showed significant improvement in the comparison between sexes.
DISCUSSION
There were no sex differences on the HAM-D before treatment initiation, but the level of improvement tended to be larger for female subjects after treatment initiation. Given the equal improvement in disease activity between male and female subjects, ADL and QOL, in addition to disease activity, may be associated with depression. The improvement in the SDAI occurred because there was no difference compared with the men. ADL have been reported to be lower for female subjects than for male subjects in many studies, but the male subjects in our study tended to engage in fewer ADL both before and after treatment initiation, and no improvement was observed.
A previous investigation of sex differences in RA reported that female subjects had higher scores for fatigue and pain in daily life than male subjects. Furthermore, in a follow-up study evaluating RA disease activity, ADL, and X-ray findings over two years according to sex, female subjects exhibited higher disease activity before treatment initiation than male subjects, and this sex difference expanded further after two years. Female subjects also displayed significantly fewer ADL [15]. In contrast, no sex differences were reported for joint X-ray findings, the CRP levels or disease activity, although female subjects engaged in fewer ADL and exhibited more severe functional disruption than male subjects. The SF-36 did not show a constant trend because some items exhibited sex differences either before or after treatment initiation [16].
Previous reports have shown that female subjects tend to have higher disease activity, but the ratio of male to female subjects in this study was extremely skewed toward female subjects, with a total sample size of 161 patients. If the sample size were larger, the results might be different. This likely occurred because there were differences between previous reports and the subject cohort in this study. Female subjects generally had better scores on the SF-36 prior to treatment initiation and then improved with treatment. “Female sex” could be defined as an adverse prognostic factor for RA in general, but “female sex” may not necessarily be considered as an adverse prognostic factor in this study.
There are several limitations to our study. First, the background characteristics were different between the men and women based on univariate analysis. Although we detected a significant difference only in HAM-D> 7 and the “mental health” item of the SF-36, we did not detect a significant difference by in disease duration, SDAI, steroid dosage or MTX dosage based on multivariate analysis. Second, the lack of statistically significant differences in men may be due to the smaller number of men than of women. Therefore, there is a possibility that this result is a false negative. Significant improvements may be observed by increasing the number of men in future studies. Third, because RA was not evaluated by X-ray, an evaluation of functional disorders that could influence ADL and QOL was not sufficiently achieved. Our follow-up period of six months is relatively short for a chronic disease such as RA; a study using an extended follow-up period might be desirable. Other factors causing differences based on sex could include the use of different drugs (the combined use of anti-rheumatoid drugs, except for methotrexate, or the combined use of non-steroid anti-inflammatory drugs), family history, prior depression, education level, social background, employment status, bereavement and support systems, levels of fatigue, pain thresholds, the influence of cytokines such as tumor necrosis factor-α and serum interleukin-6, and the influence of hormones such as dehydroepiandrosterone sulfate. Further examination will be necessary in the future to consider these factors.
CONCLUSION
We examined sex differences in RA patients using biological drugs. There were sex differences in the improvement of depressive state. When a biological drug is administered to an RA patient, it may be necessary to consider sex differences when measuring the effects because identical effects cannot be expected for male and female patients.
CONTRIBUTORS
Takahiro Tokunaga, Yusuke Miwa and Tsuyoshi Kasama planned this study and performed the statistical analyses. Yasuke Miwa is responsible for the overall content as guarantor. Airi Nishimi, Shinichiro Nishimi and Mayu Saito contributed to the methods and the discussion. Nao Oguro, Yoko Miura, Sho Ishii and Takahiro Tokunaga provided administrative support. Sanada Kenji administered the HAM-D. Tsuyoshi Kasama provided methodological advice and supervised all of the statistical procedures. All authors approved the final manuscript.
CONFLICT OF INTEREST
Yusuke Miwa received research grants from Astellas Pharm Inc., Mitsubishi Tanabe Pharma Corporation, AbbVie CK, Pfizer Japan Inc., Chugai Pharmaceutical Co., Ltd., and Eizai Co., Ltd. Tsuyoshi Kasama received research grants from Mitsubishi Tanabe Pharma Corporation and AbbVie CK. All of the other authors declare no conflicts of interest.
ACKNOWLEDGEMENTS
Declared none.
ETHICS APPROVAL
Showa University Bio-Ethical Committee (no. 742)

