All published articles of this journal are available on ScienceDirect.

Public Awareness of Rheumatoid Arthritis and Ankylosing Spondylitis in Lebanon
Authors Info & Affiliations
Abstract
Background:
Rheumatoid arthritis (RA) and ankylosing spondylitis (AS) are associated with substantial disease burdens, including impaired quality of life, functional disability, and lost productivity. Early diagnosis and effective treatment are essential to reducing disease burden and improving long-term outcomes but remain difficult to achieve.
Methods:
To better understand the deficiencies contributing to diagnostic and therapeutic delays in RA and AS in Lebanon, a computer-assisted survey of 1,200 Lebanese citizens was conducted about their awareness and knowledge of these diseases, including characteristics and management.
Results:
Approximately two-thirds and one-third of the survey participants had heard of RA and AS, respectively; two-thirds admitted they knew little about either disease after interviewers provided detailed descriptions. Most participants were aware of the major signs and symptoms of the disease, but most were unaware of serious related comorbidities and complications. While 63% identified rheumatologists as healthcare providers specializing in RA treatment, 89% indicated orthopedists were treating physicians for AS. More than three-quarters of participants understood that early treatment can be effective in RA and AS in preventing disease progression and joint damage, but two-thirds mistakenly considered treatment to be a cure. Among participants who had RA vs AS (57 [4.8%] vs 28 [2.3%]), 21.1% vs 7.1% visited a rheumatologist when initially experiencing symptoms; 64.9% vs 35.7% visited a rheumatologist for follow-up care after diagnosis.
Conclusion:
To close gaps in knowledge and management of RA and AS, initiatives are needed to raise public awareness and educate patients and healthcare providers about the importance of early diagnosis and effective treatment.
1. INTRODUCTION
Rheumatoid arthritis (RA) and ankylosing spondylitis (AS) are among the most prevalent inflammatory rheumatic diseases [1]. These closely related, progressive, life-long inflammatory diseases share many characteristics, including certain presenting symptoms, comorbidities, radiographic changes, and the potential to cause irreversible joint destruction. The disease burden for individuals and society is high, including substantial impairment of physical function and quality of life, as well as losses in household and workplace productivity [2-5]. Early diagnosis and treatment with anti-inflammatory disease-modifying drugs may improve outcomes for patients with RA and AS [6-8]. Therefore, initiatives are needed worldwide to shorten the time between symptom onset, the establishment of diagnosis, and the initiation of treatment, including early referral protocols and public awareness programs [9-11].
Understanding the perceptions and experiences of individuals in the community is critical to comprehending the deficiencies perpetuating the delayed diagnosis and treatment of RA and AS as well as formulating strategies to address them. Little published information is available about public awareness of these diseases or their management in non-Western regions such as the Middle East. To improve our understanding of the current levels of public awareness of RA and AS in Lebanon, and potentially identify educational needs, we conducted a survey of more than 1,000 members of the Lebanese public about their knowledge of RA and AS signs/symptoms, characteristics, risk factors, complications, and comorbidities. We also sought to obtain information about patients’ expectations related to the burden of disease, quality of life, disease remission, and lifestyle modifications as well as their knowledge of healthcare professionals specialized in diagnosing and managing these conditions.
2. METHODS
This nationally representative survey was conducted following a quantitative research approach, using the Collaborative Institutional Training Initiative (CITI) technique. Computer-assisted telephone interview surveys were led by eight interviewers (Statistics Lebanon Ltd.; Hazmiyeh, Lebanon), who were university students (2 men; 6 women) interested in this field of study; they had been properly trained before conducting the interview surveys and CITI certified, to avoid potential bias. Supervisors were present during the interview surveys and data collection.
The interview surveys were conducted with Lebanese citizens between March 17, 2021, and April 1st, 2021, using a questionnaire developed by Statistics Lebanon Ltd., in collaboration with the authors, to satisfy the survey objectives. The research company and its objectives were shared with participants before the interview surveys were conducted. The pilot-tested questionnaire included 40 closed-ended questions on the awareness and knowledge level of RA and AS (Supportive/Supplementary Material 1). The main themes of the survey were identified in advance of the interview surveys, i.e., public awareness and knowledge of RA and AS among people in Lebanon, which were subsequently highlighted by the survey findings.
The target sample size was 1,200 Lebanese citizens who were 18 years of age or older and resided in eight districts of Lebanon. The sample was selected as follows: 1) the available layer of the district, with counts of dwelling and clusters, was used as the first-stage sample frame; 2) probability proportionate to estimated size, a sample of the district (where the measure of size was the number of citizens by district), was used in the first stage of sample selection; and 3) a systematic choosing sample was drawn based on cluster distribution for the second stage of sampling. The sample was proportionally divided across the four historical regions of Lebanon (Beirut and Mount Lebanon, North, South, and Beqaa), rural and urban areas, as well as across age, sex, and income groups. To reach the target sample size of 1,200 citizens, the interviewers made a total of 1,437 telephone call attempts; 237 respondents declined to participate due to lack of time or interest in the subject.
The selected participants had no relationship with or knowledge of the interviewers before the survey was initiated; they were asked to take part in the interview surveys from a location in which they were alone and comfortable. Each interview survey lasted approximately 30 minutes. Interview surveys were not audio or video recorded and were not repeated; field notes were not taken by the interviewers. Participants did not receive transcripts after data collection and did not provide feedback on the survey findings.
The conduct of the study, including data collection, processing, cleaning, coding, and analysis, was overseen by Statistics Lebanon Ltd, a company specialized in conducting public opinion polls and research in Lebanon. The authors provided a description of, and one statistician was responsible for, the data coding. Data analysis was performed using SPSS statistical software (IBM SPSS Statistics for Windows, Version 20; Armonk, NY: IBM Corp). The survey data and findings were consistent.
3. RESULTS
3.1. Characteristics of the Survey Participants
The characteristics of the 1,200 individuals participating in the interview surveys are summarized in Table 1. Over the previous 12 months, prior to participating in the survey, 622 (52%) participants had not visited a health specialist or doctor. Among those who had visited a specialist or doctor in this timeframe, the largest proportion visited a general/family practitioner (21%) or a gynecologist (10%).
| Characteristic | Interviewees, %* |
|---|---|
| Age, Years | 18–75 |
|
Sex Men Women |
50.0 50.0 |
|
Marital Status Married Single |
45.4 46.0 |
|
Occupation Employed Students Homemakers Self-employed |
37.0 19.0 16.3 15.7 |
|
Education Level University degree High school diploma Vocational training Supplementary education Postgraduate degree Primary education |
45.6 20.3 12.7 10.8 6.2 3.8 |
|
Family Income/Month (LBP) 751,000–1,500,000 1,501,000–3,000,000 3,001,000–5,000,000 5,001,000–7,000,000 >7,000,000 <750,000 |
32.0 21.3 15.7 14.5 11.1 5.4 |
|
Residence Location Mount Lebanon North South Beirut Keserwen-Jbeil Bekaa Akkar Nabatieh Baalbek-Hermel |
33.3 14.2 10.8 10.0 6.7 6.7 6.7 5.8 5.8 |
| LBP, Lebanese pound. *All values are % of interviewees unless otherwise indicated. |
|
3.2. Overall Disease Awareness
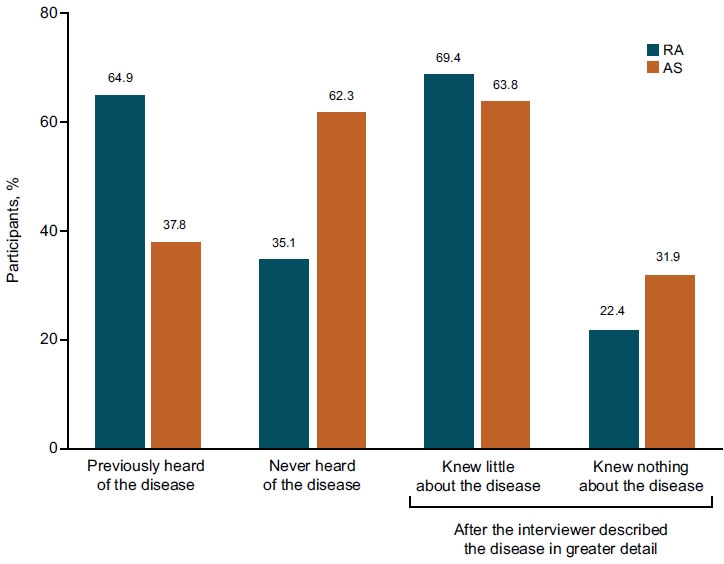
Nearly two-thirds and one-third of all survey participants had previously heard of RA and AS, respectively (Fig. 1). Among those who were aware of RA and AS, 42% and 37%, respectively, knew of the diseases because they read about them or their friends discussed them; 26% and 34%, respectively, knew of the diseases because they or a family member had the disease. Lower proportions of participants reported knowing of RA and AS through discussions with their doctors (4% and 5%, respectively).
A total of 31% and 23% of participants were familiar with RA and AS, respectively, but did not have specific knowledge about the disease. When the interviewers described RA and AS in greater detail, more than 69% and 64%, respectively, admitted that they knew little about the diseases.
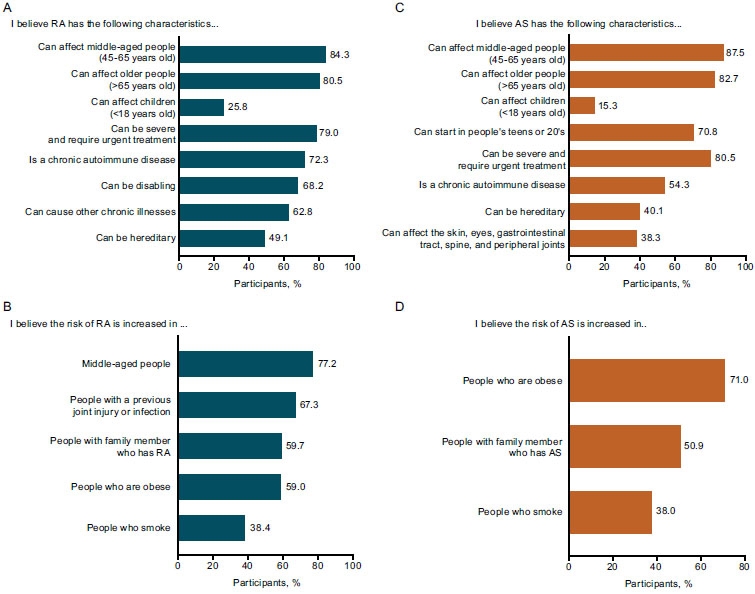
3.3. Knowledge of Disease Characteristics and Risk Factors
Findings related to participants’ knowledge of RA and AS characteristics are summarized in Fig. (2A-C). The majority of those interviewed recognized that these diseases can affect people of different ages, can be severe and require urgent treatment, and are life-long autoimmune diseases. In addition, more than half believed that RA can be disabling and can cause other prolonged diseases. However, less than half recognized the hereditary nature of RA and AS, and less than 40% understood that AS can affect the skin, eyes, gastrointestinal tract, spine, and peripheral joints.
When the interviewers inquired about the risk factors for RA (Fig. 2B, D), nearly half (49%) of the participants believed that the risk is increased in women (although they recognized the disease can affect both sexes). When asked about risk factors for AS, 39% of the participants believed men are at greater risk than women, and the same proportion believed women are at greater risk than men. Approximately three-quarters of the participants recognized that middle-aged people have an increased risk of RA, and more than two-thirds recognized previous joint injury or infection as an RA risk factor. More than half believed that the risk of RA and AS is elevated in people who have a family member with the disease or who are obese, and more than one-third identified smoking as a risk factor.
3.4. Knowledge of Disease Signs/Symptoms and Related Conditions
The survey participants were aware of several important signs and symptoms of RA, including joint pain, tenderness, swelling, and stiffness (Fig. 3A). More than two-thirds were aware that the disease can cause bone thinning and osteoporosis (83%), joint damage that may require surgery (67%), and bone erosion and joint deformities (67%). Similarly, participants were often aware of important signs and symptoms of AS, such as lower back pain and osteoporosis (Fig. 3C). In addition, a majority of participants were aware that AS can occur with osteoporosis (85%), blocked spine (82%), and inflammation in other areas of the body (63%), and can cause bone thinning and osteoporosis (80%).

In contrast, more than half of the participants were unaware that people with RA are at higher risk of developing other conditions that can substantially impair quality of life, including cancer, anemia, heart disease or diabetes, skin disorders, and mental disorders such as depression and anxiety (Fig. 3B). Many were also not aware that people with AS can experience concomitant burdensome conditions, including psoriasis, inflammatory eye and bowel disorders, and heart disease or diabetes (Fig. 3D).
3.5. Knowledge of Clinicians/Specialists and Treatment
When interviewers asked about healthcare providers who specialize in RA treatment, more than half of the participants (63%) identified rheumatologists and approximately one-third (33%) identified orthopedists as the type of physician who provides treatment for RA. In contrast, a higher proportion (89%) of participants considered orthopedists to be specialists in treating AS.
Most of those participating in the survey recognized that surgery is part of the treatment paradigm for RA and AS (83% and 81%, respectively), as is physical therapy (80% and 84%). More than three-quarters understood that many medication options are now available for these long-lasting, progressive inflammatory diseases (79% and 76%).
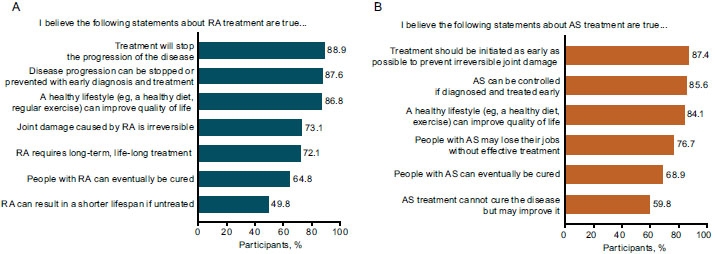
As shown in Fig. (4), approximately three-quarters of the survey participants were aware of the benefits of treatment in people with RA and AS, including its effectiveness in preventing disease progression and irreversible joint damage, and recognized that long-term treatment is needed to maintain these benefits. However, about two-thirds of those interviewed erroneously believed that people with RA and AS can be cured of the disease.
3.6. Experiences of Participants with the Disease
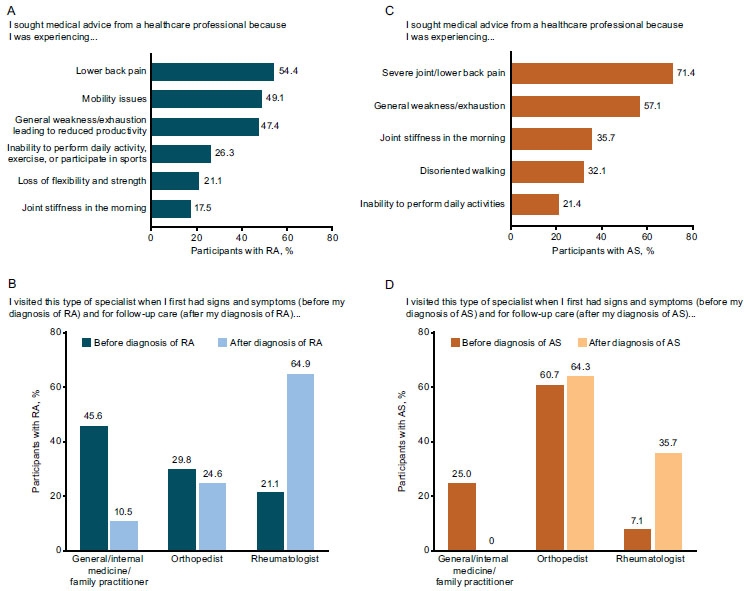
Of the 1,200 survey participants, 57 (4.8%) reported having RA, and 28 (2.3%) reported having AS. In these individuals, the most common reason for seeking medical advice from a healthcare professional was lower back pain (Fig. 5A-C). When they initially experienced symptoms, more participants with RA and AS visited general/internal medicine/family practitioners and orthopedists compared with rheumatologists (Fig. 5B, D). After receiving a diagnosis, those with RA most often visited rheumatologists for follow-up care, whereas those with AS most often continued to receive care from orthopedists.
Nearly one-third of participants with RA (29.8%) admitted that they did not change their lifestyle after receiving their RA diagnosis. However, some reported making the following lifestyle changes: adopting a special diet (38.6%), increasing their vitamin intake (38.6%), taking more time to rest and relax (35.1%), and exercising regularly (26.3%). A smaller proportion of participants with AS (14.3%) did not change their lifestyle after receiving their diagnosis, and higher proportions reported making lifestyle changes: i.e., taking more time to rest and relax (50%), increasing their vitamin intake (46.4%), exercising regularly (42.9%), and following a special diet (32.1%).
3.7. Raising Awareness via the Media
Nearly three-quarters of all survey participants (74.4%) believed it was “very important” to raise public awareness about RA and AS, whereas nearly one-quarter (23.3%) viewed it as “somewhat important”. A majority (73.6%) also reported that they were willing to attend informative sessions on RA or AS.
The participants indicated that the most effective means of raising awareness are social media (73.2%), television (59.2%), the internet (43.8%), doctors’ clinics (33.6%), billboards (22.5%), phone messages (17.7%), brochures (17.1%), and radio (15.4%). The two social media platforms with the highest response rates were Facebook (77.3%) and Instagram (11.7%).
4. DISCUSSION
When the present survey was conducted, the Lebanese healthcare system was approaching the brink of collapse [12]. After years of civil war in Lebanon, a hybrid healthcare system was established with the assistance of various laws and economic reforms [13]. Approximately half of the Lebanese population was able to acquire insurance coverage, and a large, well-trained healthcare workforce was developed, although primarily in urban areas [12]. However, these gains in the Lebanese healthcare system have recently been reversed due to the unravelling economy and the refugee crisis. A detailed description of the healthcare system in Lebanon and current strains on the system are beyond the scope of this report, but it is nonetheless important to consider this specific local backdrop when reflecting on the findings of this interview survey. While the Lebanese situation is complex and unique, as summarized below, many of the perceptions and experiences shared by this survey’s participants with chronic inflammatory disease may be generalizable to other populations worldwide.
To improve our approach to raising public awareness of RA and AS, it is essential to understand the current perceptions and experiences of individuals in the community regarding these diseases, including their beliefs about symptoms and risk factors, reasons to seek medical advice, health care providers who need to be consulted, as well as treatments and self-care. While some studies have reported such information [14-20], most have been conducted in Western countries where the culture and public health systems are very different from those in regions such as the Middle East. In the current survey conducted among Lebanese citizens, including individuals with diagnosed RA and AS, the participants displayed a relatively limited understanding of these inflammatory rheumatic diseases. While most recognized a few signs, symptoms, and complications, many lacked specific information about their characteristics and management.
The knowledge gaps exhibited in the present survey findings and elsewhere in the literature may help explain some of the major challenges associated with RA and AS patient care. Of paramount importance are the continuing delays observed in the patient’s journey to obtain a definitive diagnosis and appropriate treatment. These delays have been shown to occur at three vital stages, i.e., between the time of symptom onset and the patient’s first visit to a doctor, between the time of the first doctor’s visit and patient referral to a rheumatologist or achievement of a definitive RA diagnosis, and, finally, between the time of diagnosis and the initiation of evidence-based treatment [21]. Early diagnosis and effective treatment of RA and AS are essential to reduce the burden of the disease, improve long-term outcomes, including health-related quality of life and work productivity, and ease the patient’s journey [22].
In the literature, estimates of the time to diagnosis and treatment have varied widely, depending on factors such as when the study was conducted, and in which region, as well as the study setting, population, and design. In studies of US populations with RA performed during the latter half of the last century, the time between symptom onset and diagnosis was reported to be approximately 5 to 6 months [23, 24]. More recently, in a retrospective study in a hospital-based cohort of Venezuelan patients with RA, the average time between symptom onset and RA diagnosis was 40 months, with average delays between symptom onset and first doctor’s visit and between the first doctor’s visit and diagnosis of 16 and 24 months, respectively [25]. In an observational study conducted in Saudi Arabia, the average time between the onset of patients’ first RA symptoms and their first doctor’s visit was 6 months; a delay of about 30 months was observed from the first visit to the final RA diagnosis, with patients visiting an average of four doctors in this time span [26]. In a 2017 literature review conducted to quantify delays in RA diagnosis and treatment and related factors, Barhaimain et al. reported an average delay of 3 months between symptom onset and the first doctor’s visit, 2 months between the first visit and referral to a rheumatologist, and 3 months between rheumatologist consultation and diagnosis [21]. Patients with AS may experience even longer wait times, with average delays of 5 to 10 years reported between the onset of disease symptoms and diagnosis [27, 28]. In a German study, Feldtkeller et al. observed an average delay of 8 to 11 years between symptom onset and AS diagnosis [29]. Results of a study conducted in four countries in North Africa and the Middle East showed that the average delay from the onset of symptoms of AS to disease diagnosis was approximately 5 years [30].
Detrimental delays from the time of symptom onset or diagnosis to treatment initiation have also been reported. In the aforementioned retrospective Venezuelan study, the average time between the onset of symptoms and initiation of disease-modifying treatment was 57 months [25]. Across studies in patients with early RA conducted worldwide (i.e., in Canada, Europe, the USA, and the Middle East), the average time between disease onset and the start of disease-modifying antirheumatic treatment ranged from 6 to 18 months [31]. In the Barhamain et al. literature review, patients experienced a delay of approximately 2 months between receiving an RA diagnosis and the initiation of disease-modifying antirheumatic treatment [21]. However, in a systematic literature review and meta-analysis of the safety and efficacy of anti-tumor necrosis factor therapy in RA, which included 40 publications on 26 randomized controlled trials, the average time from diagnosis to initiation of biologic treatment ranged from 0.5 to 13 years [32]. In a large Spanish study of patients with new RA seen in a hospital setting, a delay of approximately 19 months was observed between symptom onset and initiation of the first disease-modifying therapy [33].
Several reasons have been proposed for delayed diagnosis and treatment in patients with these inflammatory rheumatic diseases. Gaps in care may start with a lack of disease awareness among individuals in the community, such as that displayed in the present survey. Approximately two-thirds of the participants in this survey indicated that they knew little about RA and AS after interviewers provided a detailed description of the diseases. Information is often shared by word of mouth, based on the experiences of friends and family, rather than medical advice shared by health care professionals. In Lebanon, delays in treatment initiation may be associated with the absence of clear governmental policies that ensure access to and continuity of treatment and support for patients, and the absence of active patient advocacy groups that can help raise patients’ voices and guarantee their rights. Patient advocacy groups play a vital role in allowing patients to share their stories and educating government officials and bodies about the need for policy or legislative changes that can have a substantial impact on their health.
Geographic/regional factors may also play a role, as patients living in rural areas have been shown to experience more prolonged delays from symptom onset to diagnosis and effective treatment compared with patients living in urban areas [26]. In Lebanon, because most rheumatologists are based in central, more urban areas of the country, patients living in peripheral, rural areas are often treated by general practitioners. This observation suggests the need for greater awareness and collaboration among general practitioners and specialists in rural areas, including potential telemedicine platforms to close this gap in care.
Delayed referral of patients with suspected RA or AS to rheumatologists can also result in a prolonged patient journey. RA and AS commonly present with nonspecific signs and symptoms in the general population, and primary care physicians and orthopedists (who often see patients first) may have difficulty in identifying patients with potential RA or AS who would benefit from prompt referral to a rheumatology specialist [30]. In a large Spanish hospital-based study of patients with new RA, a delay of approximately 17 months was reported between patients’ symptom onset and their first visit to a rheumatologist; a longer wait for treatment was associated with a delay from symptom onset to the first visit to a rheumatologist [33]. In the present survey, 75% and 86% of participants who had been diagnosed with RA and AS, respectively, visited primary care physicians and orthopedists when they initially experienced symptoms; strikingly, only 7% of those with AS had their first visit with a rheumatologist. Although participants with RA usually saw rheumatologists for follow-up care after receiving a diagnosis, those with AS most often continued to receive follow-up care from orthopedists. In the above-mentioned observational study performed in Saudi Arabia, only 3% of patients with RA initially sought to visit a rheumatologist, whereas 91% sought consultation with general practitioners or orthopedists [26]. Non-rheumatologists provided the diagnosis in 24% of patients, whereas rheumatologists provided the diagnosis in the remaining 76%. In a Venezuelan retrospective study, 92% of patients with RA received a definitive diagnosis from a rheumatologist [25]. However, longer times to diagnosis and initiation of disease-modifying antirheumatic treatment were associated with first visits to primary care physicians or orthopedists, suggesting that gaps in care are also triggered by patient visits to these practitioners.
In Lebanon, as in other regions, several actions are needed in the future to address the challenges facing patients with RA and AS and health care providers. Public awareness of disease symptoms, the need for early diagnosis and treatment, and the importance of rheumatology specialists may be enhanced via social media campaigns, live community events with professional and patient speakers sharing their knowledge and experiences, and patient support/advocacy group activities. At a national level, government officials and bodies need to be engaged and public awareness campaigns developed and implemented. The creation of rheumatology clinics in government hospitals and primary healthcare centers in rural areas of Lebanon is widely supported by experts in this field to allow access to a high quality of care for patients who cannot afford the cost of private medicine, which is dominant in Lebanon. This is particularly important due to the current economic crisis in Lebanon, as many patients are unable to afford private clinics. Moreover, nurses in primary healthcare centers (especially in rural areas) require additional education on the diagnosis of inflammatory rheumatic diseases such as RA and AS to help improve timely diagnosis remotely via telemedicine platforms with clinical specialists.
In this survey, many participants suggested that knowledge can be disseminated on television, on the internet, and at doctors’ clinics. Greater public awareness of RA and AS will bring greater understanding and acceptance of patients with these debilitating life-long diseases, which traditionally have not received adequate attention. For individuals who have not yet been diagnosed, such awareness will help them recognize their symptoms and communicate more clearly and knowledgeably with their doctor, potentially reducing the delay between symptom onset and RA and AS diagnosis. In addition, improvements in the public’s understanding of RA and AS can help those affected discuss the disease more freely and publicly without shame, form stronger partnerships with their healthcare providers, and become more engaged in society. Greater disease awareness and knowledge may also enhance the recognition of patients’ rights, both in the community and at work, and improve access to important tools, such as patient hotlines, patient advocacy groups, physiotherapy, dieticians, and mental health support.
With the ongoing economic crisis in Lebanon, private health care has become prohibitively costly, and essential medicines, such as biologics used to treat long-lasting inflammatory diseases, are in very short supply. In this situation, patient support/advocacy groups play a particularly important role in empowering patients, who have a critical need for medical treatment, mental health support, and physiotherapy, in their interactions with government and regulatory authorities. Educational activities are needed to address the barriers that prevent patients from seeking appropriate medical treatment despite the consequences to their health.
Although not a topic addressed in this survey, unmet educational needs also exist for healthcare providers in the region. For example, teaching primary care physicians, orthopedists, and physiotherapists how to recognize inflammatory rheumatic diseases early would help reduce the time from symptom onset to rheumatologist referral and definitive diagnosis. Reinforcing their knowledge of referral strategies would also diminish these delays. Finally, continuing medical education for rheumatologists focused on the importance of early diagnosis and effective treatment may also be beneficial in ensuring optimal management of patients with RA and AS in the future.
CONCLUSION
Based on the findings of our survey conducted in Lebanon to improve the understanding of people’s perceptions and experiences related to the rheumatic diseases RA and AS, nearly two-thirds of participants were aware of RA and AS, but a similar proportion admitted they knew little about the diseases. Although most participants identified major signs and symptoms of the diseases, most were unable to identify serious related comorbidities and complications. The essential role played by rheumatologists as specialists in RA and AS, both at symptom onset and for follow-up care, appeared to be underrecognized by survey participants, including those who had been diagnosed with the disease. These findings highlight the current need for initiatives to help raise public awareness of RA and AS and educate the community and healthcare providers about the importance of early diagnosis and effective treatment and close existing gaps in the understanding and management of the diseases.
AUTHORS' CONTRIBUTION
All authors satisfied the authorship criteria established by the International Committee of Medical Journal Editors (ICMJE) [34]. Specifically, Jeanine Menassa and Marcelle Ghoubar made substantial contributions to the conception and design of the interview survey; Jeanine Menassa, Essam El Naggar, Nancy Sunna, and Marcelle Ghoubar Dima Bou Nassar made substantial contributions to the conception and design of the manuscript; all authors made substantial contributions to the acquisition, analysis, or interpretation of the survey data and drafting or revising the work; and all authors provided final approval of the manuscript version submitted for publication and agreed to be accountable for the work.
LIST OF ABBREVIATIONS
| RA | = Rheumatoid arthritis |
| AS | = Ankylosing spondylitis |
| CITI | = Collaborative Institutional Training Initiative |
ETHICAL STATEMENT
Ethical standards (the Market Research Society Code of Conduct) were followed respecting the privacy, protection, and anonymity of all participants in the survey, and their informed oral consent was obtained prior to their participation. Lebanon does not require national ethics approval for public surveys. As the present research was conducted as a public survey, it also does not require any local/private Institutional Review Board approval.
CONSENT FOR PUBLICATION
Informed consent was obtained from all participants.
STANDARDS OF REPORTING
COREQ guidelines were followed.
AVAILABILITY OF DATA AND MATERIALS
The data supporting this article’s findings are available within the article.
FUNDING
This study was sponsored by Pfizer. Medical writing support for this manuscript was provided by Donna McGuire of Engage Scientific Solutions and was funded by Pfizer.
CONFLICT OF INTEREST
Jeanine Menassa, Dima Bou Nassar, and Farah Naboulsi have no conflicts of interest to disclose. Essam El Naggar, Nancy Sunna, and Marcelle Ghoubar are employees of Pfizer and hold stock and/or stock options with Pfizer.
ACKNOWLEDGEMENTS
The authors would like to thank the individuals who participated in this research initiative.
SUPPLEMENTARY MATERIAL
Supportive/Supplementary Material 1. Interview survey questionnaire. Supplementary material is available on the Publisher’s website.

