All published articles of this journal are available on ScienceDirect.

The Diagnostic Significance of Serum Sclerostin in Early Detection of Rheumatoid Arthritis in Syrian Patients
Abstract
Background:
Rheumatoid arthritis (RA) is associated with joint deformities and local bone erosions. Sclerostin is an inhibitor of the Wnt pathway and drives to reduce bone formation.
Aims:
Our study aimed to compare the diagnostic significance of sclerostin with anti-CCP (anti-cyclic citrullinated peptide; normal level<20 IU/ml, and rheumatoid factor (RF; normal level<16 IU/ml) for the early diagnosis of rheumatoid arthritis in Syrian patients.
Methods:
This study contained fifty-eight RA patients and thirty healthy individuals who were equally age- and sex-matched. Serum sclerostin and serum anti-CCP (IgG) levels were evaluated by using the enzyme-linked immunosorbent assay (ELISA). RA activity was assessed based on disease activity scores (DAS28).
Results:
Our results indicated that serum levels of sclerostin levels were higher in the RA group than in the healthy group (p<0.001). There was a positive correlation between serum sclerostin and DAS28-ESR (r=0.413, p=0.001). By ROC curve, the most optimal cut-off value of sclerostin was 249.69 pg/ml (AUC was 0.910 with 95% confidence interval (CI) values (0.852-0.969), sensitivity of 87.9%, and specificity of 93.3%) [Odds Ratio (OR) and P-value: 102, P< 0.0001]. In RA patients, the sensitivity and specificity of anti-CCP were 74.1% and 90%, and 70.6% and 86.6% of RF, respectively.
Conclusion:
Increased serum sclerostin may aid as a new prognostic biomarker for evaluating the activity of RA. Sclerostin showed higher sensitivity and specificity than anti-CCP and RF-IgM antibodies. Therefore, sclerostin is a sensitive and specific biomarker for early diagnosis of rheumatoid arthritis.
1. INTRODUCTION
Rheumatoid arthritis (RA) is a chronic autoimmune disorder with an estimated prevalence of 0.3-1% in 2018 in the general population [1, 2]. However, women are affected two to three times more often than men. It is characterized by symmetrical synovial inflammation, pannus formation, advanced joint destruction, and bone erosions [3, 4]. If the disease is not controlled and diagnosed in an early stage, it will lead to severe irreversible outcomes, such as joint impairment and functional disability [3, 5]. Early diagnosis and the initiation of aggressive treatment are the most significant stages in decreasing the disease progression and joint destruction [6, 7]. To date, there is no single reliable laboratory test for the diagnosis of rheumatoid arthritis [8]. Presently, the diagnostic parameters have relied upon American College of Rheumatology (ACR 2010) criteria, which include acute phase reactants, such as erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and autoantibodies like rheumatoid factor (RF) and anti-cyclic citrullinated peptide antibodies (ACPAs) [9]. For RA diagnosis, the sensitivity and specificity of ACPA were 67% and 95%, respectively [10]. The sensitivity of RF does not exceed 79%, and the specificity is about 84% [11]. ACPAs can be present in some pathological cases, such as tuberculosis [8, 12, 13]. In addition, RF antibodies can be found in some infections and autoimmune diseases, and they appear in healthy individuals (specificity 85%). On the other hand, approximately 31% of RA patients are RF seronegative, and about 33% of RA patients are assessed as ACPA-seronegative [8, 14]. As for acute phase markers, ESR and CRP are inflammatory indicators, but they are not specific in rheumatoid arthritis and are affected by several factors [14, 15]. So, there is a critical necessity to explore alternative new biomarkers besides the traditional prognostic factors that may help to assess disease activity, confirm the early diagnosis, identify high-risk patients, and allow the start of intensive therapy [4, 8].
Recent research has focused on some biomarkers that play a prominent role in the pathogenesis of RA and shed light on sclerostin (SOST) as an antagonist of the wingless (Wnt) signaling pathway [16, 17]. The Wnt/β-catenin pathway is important in the control of osteoblast differentiation leading to bone formation [18, 19]. It is triggered by the binding of Wnt proteins to receptor complexes collected from frizzled receptor proteins (FRPs) and co-receptors called low-density lipoprotein receptor-related protein families 5 and 6 (LRP-5 and LRP-6), leading to raised levels of cytosolic β-catenin. As a next step, β-catenin stabilization, nuclear translocation, and motivation of goal genes occur that promote osteoblast differentiation [20, 21]. Inhibition of the Wnt/β-catenin pathway by sclerostin contributes to the bone loss mechanism in rheumatoid arthritis [22, 23]. Sclerostin is a glycoprotein and a product of the SOST gene and is situated on the 17q12-q21 chromosome [24, 25]. It is not only secreted from osteocytes but also by other cells, such as chondrocytes and cementocytes, as well as from the kidney and liver [19, 24]. It inhibits the Wnt pathway by its binding to the LRP-5/LRP-6, which blocks the formation of a complex consisting of (FRPs) and its co-receptors, resulting in the activation of intracellular β-catenin dissolution and preventing its translocation to the nucleus [21, 26]. Sclerostin is involved in impaired bone repair in rheumatoid arthritis by supporting osteoclast activity and osteoblast blocking, thereby inhibiting the production of bone [16, 26, 27]. In addition to its role, it boosts the secretion of receptor activator of nuclear factor κB ligand (RANKL) from osteocytes and decreases the expression of osteoprotegerin (OPG) [16, 27]. Several recent studies have revealed the importance of assaying serum levels of sclerostin and confirmed an increase in these levels in RA patients [16, 17, 28] and its association with RA activity [17, 29]. The purpose of our research was to estimate the serum sclerostin levels, the pertinence between these levels, and the parameters of rheumatoid arthritis activity and to examine whether this serum biomarker may be practical in combination with other prognostic factors in rheumatoid arthritis.
2. MATERIALS AND METHODS
Our cross-sectional study was completed from January 2020 to May 2021 and composed of eighty-eight individuals divided into two groups: the first group was the RA patients group consisting of 58 patients (47 females and 11 males), with a mean age of 48.71 ± 10.45 years and ranging from 28 to 65 years. The second one was the healthy group that included 30 individuals (7 males and 23 females) of age- and sex-matched. Their mean age was 46.17 ± 10.94 years. The sample size in our study was determined based on the cost, time, or convenience of data collection and the need to provide adequate statistical power. Rheumatoid arthritis was diagnosed by rheumatologists in the Rheumatology Clinic of Al-Mowasat Hospital, Almoujtahed Hospital, according to the ACR 2010/EULAR criteria. The duration of the symptoms was less than two years.
Inclusion criteria included newly diagnosed with rheumatoid arthritis and naïve disease-modifying antirheumatic drugs (DMARDs) patients. While the exclusion criteria were the patients with the following conditions: renal or cardiac diseases, liver disease, nephrotic syndrome, Cushing syndrome, additional autoimmune diseases, such as systemic lupus erythematosus (SLE), secondary causes of osteoporosis, and patients taking treatment that affects bone mineral density (BMD) (e.g., estrogen, steroids).
Laboratory tests contained complete blood count (CBC), C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), Rheumatoid factor (RF) by latex agglutination, and anti-cyclic citrullinated peptide (anti-CCP), accomplished by ELISA method. RF rates >15 IU/ml and anti-CCP rates > 20 IU/ml were estimated positive. All results of these data were taken and gathered from patients’ files at diagnosis.
The disease activity was evaluated depending on (DAS28) examining ESR, number of swollen joint count (SJC), tender joint count (TJC), and patient's global assessment, then DAS28ESR was designed as:
DAS28-ESR = 0.56√ (TJC28) + 0.28√ (SJC28) + 0.70 Ln (ESR) + 0.014 (GH) [30]. RA patients were divided into several groups consistent with DAS28ESR; patients with DAS28 > 5.1 were categorized as high disease activity, patients with DAS28 >3.2 and ≤ 5.1 were labeled as modest disease activity, patients with DAS28 ≥ 2.6 and < 3.2 were classified as little disease activity, and if DAS28 was <2.6, then patients were in the remission stage.
2.1. Sampling
Serum blood samples were collected in the period between May 2020 and September 2021, centrifuged at 4000 rpm for 10 minutes, and then the serum was distributed into four Eppendorf tubes. Samples were kept at -80 °C until the assays were performed.
Serum sclerostin levels were measured by ELISA technique using the commercial kit (Boster Picokine™ Technology, Germany) with intra-assay and inter-assay coefficients of variation (CV%), i.e., 6.7% and 7.7%, respectively. The detection range was 31.5 to 2,000 pg/mL, with a sensitivity of <10 pg/ml.
2.2. Ethical Approval
The approval was obtained by the Scientific Research Ethics Committee at Damascus University, as mentioned in session No. 3, February 2019/2020. Informed consent was obtained from all study participants.
2.3. Data Quality Assurance
The study data was collected by interview questionnaire for all participants. The rheumatologist supervised the data and recorded it in patients' files, which had been gathered to complete the data on a daily practice. Informed written consent was obtained after the elucidation of the aim of the study. Ethical deliberations were obtained according to the principles of the Helsinki Declaration.
2.4. Statistical Analysis
Data handling was achieved using Statistical Package for the Social Sciences (SPSS) version 25 and MS Excel (Microsoft Office Excel 2019). Continuous variables were offered as mean and standard deviation (SD), and frequencies and percentages were used to define categorical variables. The Kolmogorov-Smirnov test was used for the normality of the distribution (sclerostin values were non-normally distributed). Differences between the two independent groups were assessed by the Mann–Whitney U test. Spearman’s correlation coefficient was applied to describe the relationship between the two variables. The Chi-square test was used for the comparison of variables, including categorical data. The ROC curve (receiver operating characteristic) was used to limit the diagnostic cut-off of sclerostin, RF, and anti-CCP and assess their sensitivity and specificity in RA diagnosis. Positive predictive value (PPV) and negative present value (NPV) were calculated. P-value < 0.05 was adopted as statistically significant.
3. RESULTS
There were 19% (N=11) males and 81% females (N=47) in the RA patients’ group, while the healthy group included 23.3% (N=7) males and 76.6% (N=23) females. Moreover, 35% (N=16) of RA patients were females, and 34.7% (N=8) of healthy group females were in menopause. Moreover, 82.8% (N=48) of patients were either RF or ACPA positive, 42 (72.5%) were both RF and ACPA positive, and 29.9% (N=15) of them had articular deformities. Table 1 presents the results of laboratory tests of RA group patients.
| Variables | Mean ± SD | Range (Min, Max) |
|---|---|---|
| Age (years) | 48.71 ± 10.45 | 43 (24 - 67) |
| Hb (g/dl) | 11.94 ± 1.18 | 6.1 (8.9 -15) |
| WBC (x103/mm3) | 8.11 ± 2.09 | 9.3 (3.5 - 12.8) |
| Calcium (mg/dl) | 8.88 ± 0.74 | 3.9 (6.10- 10) |
| DAS28-ESR | 5.39 ± 0.98 | 4.23 (7.4 - 3.17) |
| ESR (mm/h) | 44.79 ± 16.62 | 65 (10- 75) |
| CRP (mg/L) | 20.55 ± 22.66 | 105.8 (0.2 - 106) |
| VAS (%) | 0.67 ± 0.20 | 0.80 (0.2 - 1.0) |
| TJC | 9.66 ± 4.56 | 18 (2 - 20) |
| SJC | 5.43 ± 2.60 | 12 (0 - 12) |
| RF (IU/ml) | 121.47 ± 133.78 | 706 (4 - 710) |
| Anti-CCP (U/ml) | 375.02 ± 345.75 | 1316.5 (3.50 - 1320.0) |
| Symptom’s duration (months) | 8.05 ± 3.63 | 13 (3 - 16) |
According to DAS28, ESR patients were classified: 34 (58.6%) of them were of high disease activity, 22 (37.9%) had moderate disease activity, and two patients (3.5%) had low disease activity.
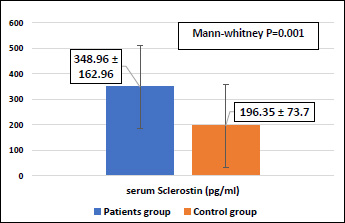
Our study found an increase in the mean of serum sclerostin levels (348.96 ± 162.96 pg/ml), which ranged from 75.91 to 895.2 pg/ml in RA patients compared to the healthy group (196.35 ± 73.7 pg/ml), in which levels ranged from 102.77 to 345.39 pg/ml. By applying the Mann-Whitney test, a statistically significant difference (P=0.001) was observed between the two groups, as shown in Fig. (1).
Our results demonstrated that serum sclerostin levels correlated positively with DAS28-ESR (r=0.413, p=0.001) (Fig. 2).
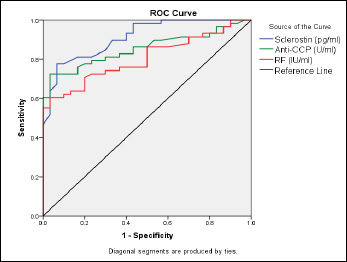
The ROC curve analysis showed that the best cut-off value of serum sclerostin was 249.69 pg/ml (sensitivity (87.9%) and specificity (93.3%)), which was the highest. The AUC with 95% CI was 0.910 [ Odds Ratio (OR) and 95% CI and P-value: 102 (19.8 to 524.6), P< 0.0001] to distinguish between patients and healthy groups (Table 2, Fig. 3). Our results presented that 53 (51 true positives, 2 false positives) were sclerostin positive, and 35 (28 true negatives, 7 false negatives) were sclerostin negative according to the cut-off value of sclerostin (Table 3).

| Test Result Variable(s): Serum Sclerostin (pg/ml) | ||||
|---|---|---|---|---|
| Area Under the Curve | Std. Errora | Asymptotic Sig.b | Asymptotic 95% Confidence Interval | |
| Lower Bound | Upper Bound | |||
| 0.910 | 0.030 | p<0.001 | 0.852 | 0.969 |
| - | RA Patients | Control Group | All Participants | Chi-square P-value |
|---|---|---|---|---|
| Positive (Sclerostin) | 51 | 2 | 53 | P<0.001 |
| Negative (Sclerostin) | 7 | 28 | 35 | |
| - | 58 | 30 | 88 | - |
| AUC | Sensitivity | Specificity | Cut-off | PPV | NPV | OR | Biomarker |
|---|---|---|---|---|---|---|---|
| 0.854 | 74.1 | 90% | 15.20 | 93.3 | 62.7 | 23.6 | Anti-CCP (U/ml) |
| 0.804 | 70.6 | 86.6 | 7.93 | 91.1 | 60.4 | 15.6 | RF (IU/ml) |
| 0.910 | 87% | 93.3% | 249.69 | 96.2% | 80% | 102 | Sclerostin (pg/ml) |
The ROC curve analysis produced the AUC (0.804 and 0.850) for RF and anti-CCP, respectively (Fig. 3). Table 4 presents that the sensitivities of RF and anti-CCP were 70.6% and 74.1% at an early disease stage with cut-off values of 7.93 and 15.20 with a specificity of 86.6% and 90%, respectively.
4. DISCUSSION
Rheumatoid arthritis is associated with the emergence of irreversible bone erosions, joint deformities, and bone density loss. They occur in two-thirds of RA patients due to the increased mechanism of bone resorption in this disease [28, 31]. We have highlighted an inhibitor of the Wnt pathway, sclerostin, that plays a prominent role in the inflammatory bone resorption mechanism in RA patients [17]. Our study found an increase in serum sclerostin in RA patients related to the healthy group (P= 0.001). The reason for this elevation is due to the effect of inflammatory cytokines, which leads to the increased expression of sclerostin and its production by osteoblasts [32]. On the other hand, TNF-α stimulates osteoclasts and leads to an increase in the expression of DKK-1, another inhibitor of the Wnt pathway, and plays a vital role in the stimulation of sclerostin production [16, 25, 29]. This is confirmed by several studies, such as the study by El-Bakry et al. in Egypt, which included 31 RA patients and reported increased serum sclerostin levels compared to 10 healthy controls [31]. Moreover, Gharbia et al. conducted a study on 40 RA patients and 40 control persons [17], and Aydemir et al. conducted a study in Turkey that comprised 60 RA patients and 30 controls [22]. All of these studies found that serum sclerostin levels in RA patients were significantly higher than in controls. Conversely, there was no change in sclerostin levels among RA patients and the healthy group in several studies. The cause for this inconsistency may be due to the diverse stages of disease in which the serum samples were taken. In addition, RA patients in these studies were of low disease activity or in the stage of clinical remission [32, 33]. Furthermore, in 2015, in a study by Vargas et al. in Mexico on 48 RA patients and 15 healthy controls, 50.98% of the RA patients were in clinical remission, so they confirmed that there is no intervention of sclerostin in RA pathogenesis [1].
Our study has reported that serum sclerostin levels were completely associated with DAS28 (r=0.413, p=0.001). The same finding in the correlation of sclerostin levels with DAS28 was observed by El-Bakry in India [31], a Gharbia study in Egypt [17], and Megid et al., which contained 50 RA patients and 20 healthy persons [34]. All these studies presented that the levels of serum sclerostin were significantly related to RA disease activity at the early stage. Thus, monitoring the disease activity is the main feature for corrective local and systemic bone health in RA patients [17, 29].
The study by Aydemir et al. in Turkey in 2020 on 60 RA patients did not find an association between serum sclerostin levels with RA activity, and this could be explained by the fact that the patients participating in the study were in the late phase of RA [22]. Moreover, the study by Mehaney et al. in 2015 found that there was no correlation between sclerostin levels and DAS28. This may maybe because only three (7.5%) of 40 newly diagnosed RA patients were not receiving any specific therapy, and 70% of patients were using methotrexate [33].
The ROC curve analysis presented that the best cut-off concentration of serum sclerostin was 249.69 pg/ml (sensitivity, 87.9%; specificity, 93.3%). The study by El-Bakry et al. showed that serum sclerostin levels of 267ng/dl, a sensitivity of 96.8%, and a specificity of 66.7% [31] were recorded. In the study by Shawky Alashkar in 2022 conducted on 80 early patients, the sensitivity and specificity of anti-CCP were 68.3%, 95%, and 61.7%, 88.3% for RF antibodies, respectively [35]. The 2019 study by Singh et al. in India demonstrated that at a value of 394 pg/ml, the sensitivity was 100%, the specificity was 90%, PPV was 90%, and NPV was 100% to differentiate the group of rheumatoid arthritis patients from the healthy group [24]. All of these studies, including ours, propose the role of sclerostin in RA pathogenesis and the importance of its serum levels as a potential new biomarker in the diagnosis and evaluation of disease activity. Our study investigated that sclerostin is better as a diagnostic biomarker of the disease than anti-CCP and RF.
The strength of our study is that the sclerostin levels are measured in the early stage of RA before the treatment by a high-sensitivity ELISA technique. The limitations of our research include the small sample size of patients and a lack of other bone turnover biomarkers. Not measuring serum sclerostin several times and not knowing the effect of treatment and its importance in evaluating the therapeutic response are also some of the limitations of our study. However, the overall consequences of the present study are normally coordinated and are consistent with many previous studies. It would be much more reliable if we avoided some limitations.
CONCLUSION
In this study, sclerostin showed higher sensitivity and specificity than anti-CCP and RF-IgM antibodies; therefore, sclerostin is a sensitive and specific biomarker for early diagnosis of rheumatoid arthritis. Moreover, increased levels of sclerostin are associated with RA activity, which highly suggests that it may play a role in the pathogenesis of RA, thus making it a valuable novel biomarker for monitoring the progress of the disease.
LIST OF ABBREVIATIONS
| ELISA | = Enzyme-linked Immunosorbent Assay |
| CI | = Confidence Interval |
| RA | = Rheumatoid Arthritis |
| DMARDs | = Disease-modifying Antirheumatic Drugs |
| BMD | = Bone Mineral Density |
| SLE | = Systemic Lupus Erythematosus |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The approval of the Ethics Committee was obtained by the Scientific Research Ethics Committee at Damascus University, as mentioned in session No. 3, February 2019/2020.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent was obtained from all participants.
STANDARDS OF REPORTING
STROBE guidelines were followed.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available in google drive on: https://docs.google.com/spreadsheets/d/11S3I9RtXOcBWfcu2lhYAaigJiOIIiQQ_/edit?usp=drivesdk&ouid=111648084332255373994&rtpof=true&sd=true
FUNDING
This research is funded by Damascus University-funder No.501100020595.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGMENTS
The authors would like to thank Dr. Saha Al Shamma, Ph.D. in biochemistry, for her valuable comments about the manuscript, Dr. Imad Al Dean Al Masri for his useful advice and help in the statistical analysis program, and Rheumatologist Dr. Hytham Pirkdar for facilitating in the collection of RA patients’ samples.

